Ahead of the now delayed publication of the NHS operating framework and as integrated care systems (ICSs) mark their first full year running as key NHS statutory bodies in 2023/24, WA Communications has undertaken a first of its kind in-depth analysis of all 42 ICBs annual accounts.
This analysis, the second in our ‘the state of ICSs’ series, following our ICB five-year forward plans data map, has been created to foster a mutual understanding of the challenges and opportunities that exist within the NHS, supporting strong collaboration between the private, third sector and ICBs.
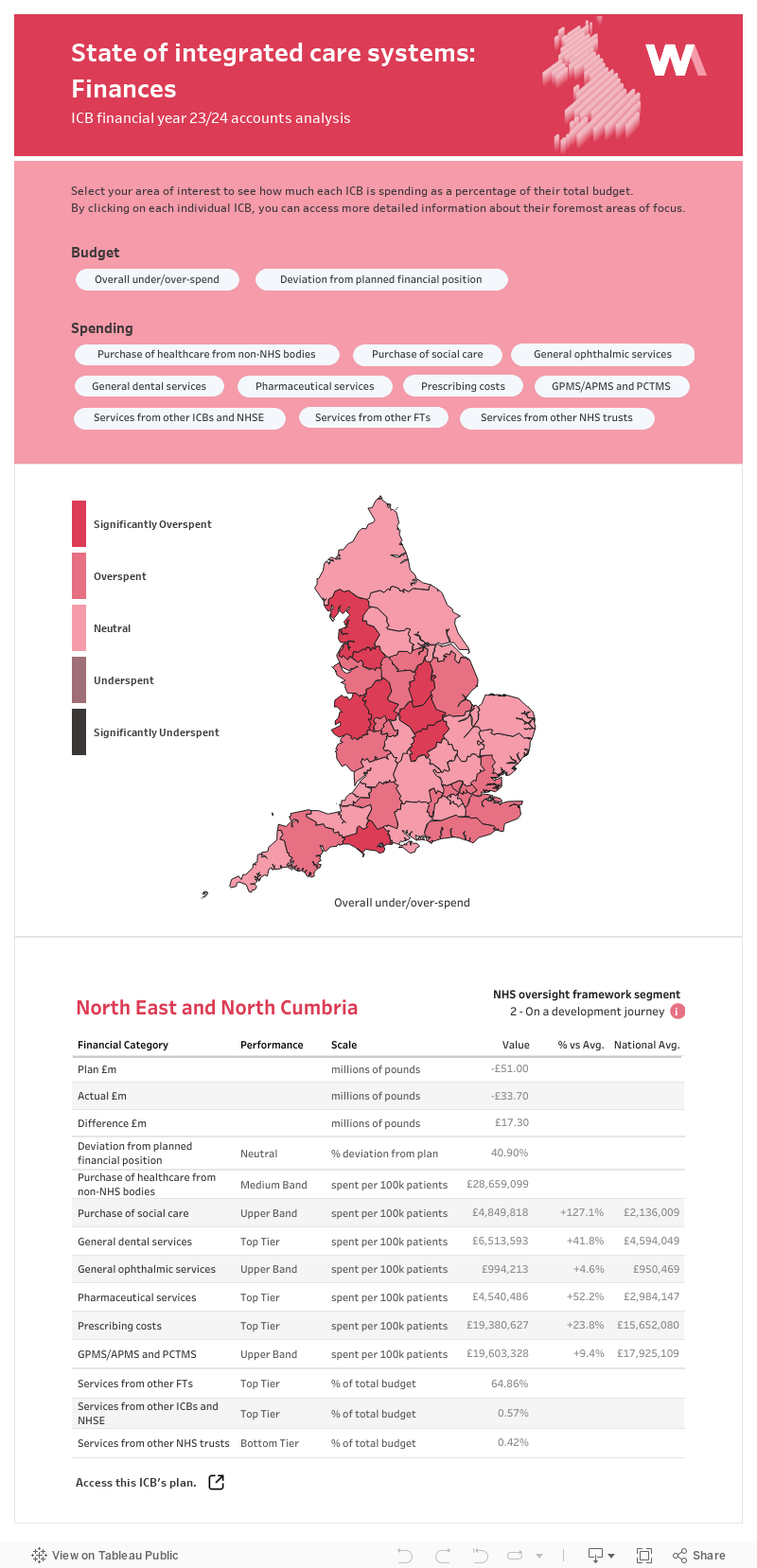
We have taken the published accounts and produced an interactive ICB Spending Map that enables comparisons of financial performance – not just of total spend, but more valuable analysis of category spend against the budget set and as a percentage of each ICB’s total budget. In this way comparisons can be made within and across ICBs around the spend upon key categories such as acute hospital care, mental health services and primary care prescribing.
We launch our analysis at a time where ICBs are being asked to take on increasing amounts of responsibility while being scrutinised over finances and impact more than ever:
- ICBs are already the lead NHS bodies for strategy and spend.
- The delegation of specialised services commissioning and budgets has recently been reinforced and will add to the value of future versions of this map, but also increases the range of organisations needing to focus upon differential ICB performance.
- NHS policy is placing increasing importance upon local interpretation of national priorities through ICB-led population health management.
- The imminent NHS Ten Year Forward Plan is expected to further develop devolution of priority-setting and spend, possibly through new integration with elected Mayors and other regional local authorities.
- 18 of the 42 ICBs are currently subject to NHSE’s investigation and intervention programme, meaning they are in financial turnaround monitoring with externally imposed oversight of their overspending.
Methodology
The interactive map uses colour-coded visuals to highlight performance against stated budget, ranking ICBs from significantly overspent through to significantly underspent.
By comparing average figures by 100,000 patient populations we have been able to more accurately compare ICBs. This is important given that ICBs vary so much in gross population with the largest being more than five times larger in population than the smallest.
ICB budgets are set upon a set of formulas that are based upon the number of people registered as patients at their host GP practices. A complex set of weighted capitation indexes then set their baseline budgets through detailed assessment of relative health need against primary care, secondary care and specialised services variables. This produces a highly varied per capita baseline position that needs to be take into account to understand spend performance.
Data map
Our five key takeaways
- There are emerging patterns of comparisons that indicate a polarising trend across the ICBs linked to factors such as ICB inheritance of historic local trends, presence of major tertiary centres and performance of local acute hospitals.
- The impact of the weighted capitation formulas is pivotal and provides a clear pattern of correlations with overall financial status.
- However, there are notable exceptions to the above as Greater Manchester ICB, for example, is both highly capitated and significantly overspent.
- Therefore, the percentage spend by an ICB on acute hospital services and the level of under/over spend of this category is a key differentiator in overall ICB performance, which reflects a fundamental tension in the NHS structural relationship of ICB to NHS FT/trust control.
- Primary care prescribing costs are the greatest true variable cost to an ICB and a consistent category of overspending.
About WA Communications
WA Communications is an integrated strategic communications and public affairs consultancy. Our specialist health practice supports clients across a diverse range of diseases at the intersection of policy, government affairs and communications, to achieve their strategic objectives.
If you would like to discuss how to best work in partnership with Integrated Care Systems, and our analysis of their comparable financial performance, contact Lloyd Tingley at lloydtingley@wacomms.co.uk.
